Fat-Soluble Vitamins
University of Hawai‘i at Mānoa Food Science and Human Nutrition Program and Human Nutrition Program
Vitamin A Functions and Health Benefits
is a generic term for a group of similar compounds called . is the form of vitamin A found in animal-derived foods, and is converted in the body to the biologically active forms of vitamin A: and retinoic acid (thus retinol is sometimes referred to as “preformed vitamin A”). About 10 percent of plant-derived , including , can be converted in the body to retinoids and are another source of functional vitamin A. Carotenoids are pigments synthesized by plants that give them their yellow, orange, and red color. Over six hundred carotenoids have been identified and, with just a few exceptions, all are found in the plant kingdom. There are two classes of carotenoids—the xanthophylls, which contain oxygen, and the carotenes, which do not.
In plants, carotenoids absorb light for use in photosynthesis and act as antioxidants. Beta-carotene, , and are converted to some extent to retinol in the body. The other carotenoids, such as lycopene, are not. Many biological actions of carotenoids are attributed to their activity, but they likely act by other mechanisms, too.
Vitamin A is and is packaged into in small intestine, and transported to the liver. The liver stores and exports vitamin A as needed; it is released into the blood bound to a , which transports it to cells. Carotenoids are not absorbed as well as vitamin A, but similar to vitamin A, they do require fat in the meal for absorption. In intestinal cells, carotenoids are packaged into the lipid-containing chylomicrons inside small intestine mucosal cells and then transported to the liver. In the liver, carotenoids are repackaged into lipoproteins, which transport them to cells.
The retinoids are aptly named as their most notable function is in the retina of the eye where they aid in vision, particularly in seeing under low-light conditions. This is why is the most definitive sign of vitamin A deficiency.Vitamin A has several important functions in the body, including maintaining vision and a healthy immune system. Many of vitamin A’s functions in the body are similar to the functions of hormones (for example, vitamin A can interact with DNA, causing a change in protein function). Vitamin A assists in maintaining healthy skin and the linings and coverings of tissues; it also regulates growth and development. As an antioxidant, vitamin A protects cellular membranes, helps in maintaining levels, and influences the amount and activity of enzymes that detoxify .
Vision
Retinol that is circulating in the blood is taken up by cells in the eye retina, where it is converted to retinal and is used to help the pigment rhodopsin, which is involved in the eye’s ability to see under low light conditions. A deficiency in vitamin A thus results in less rhodopsin and a decrease in the detection of low-level light, a condition referred to as night-blindness.
Insufficient intake of dietary vitamin A over time can also cause complete vision loss. In fact, vitamin A deficiency is the number one cause of preventable blindness worldwide. Vitamin A not only supports the vision function of eyes but also maintains the coverings and linings of the eyes. Vitamin A deficiency can lead to the dysfunction of the linings and coverings of the eye (eg. bitot spots), causing dryness of the eyes, a condition called . The progression of this condition can cause ulceration of the cornea and eventually blindness.
Figure 9.3 Bitot Spot caused by vitamin A deficiency

Figure 9.4 Vitamin A Deficiency World Map
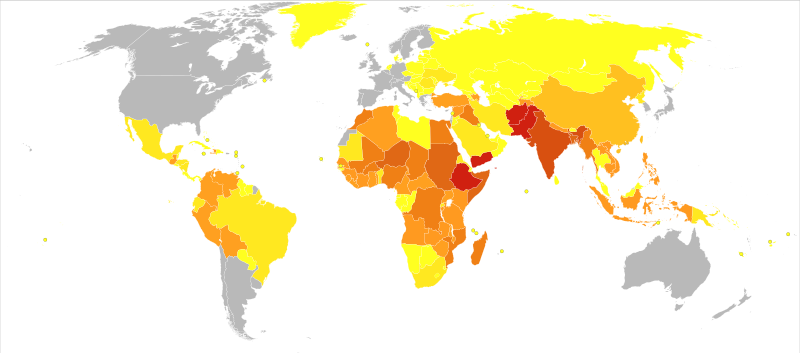
| 0-28 | 31-78 | 85-85 | 85-141 | 144-257 | 258-376 | 432-455 | 558-558 | 586-883 |
Immunity
The common occurrence of advanced xerophthalmia in children who died from infectious diseases led scientists to hypothesize that supplementing vitamin A in the diet for children with xerophthalmia might reduce disease-related mortality. In Asia in the late 1980s, targeted populations of children were administered vitamin A supplements, and the death rates from measles and diarrhea declined by up to 50 percent. Vitamin A supplementation in these deficient populations did not reduce the number of children who contracted these diseases, but it did decrease the severity of the diseases so that they were no longer fatal. Soon after the results of these studies were communicated to the rest of the world, the World Health Organization (WHO) and the United Nations Children’s Fund (UNICEF) commenced worldwide campaigns against vitamin A deficiency. UNICEF estimates that the distribution of over half a billion vitamin A capsules prevents 350,000 childhood deaths annually.[1]
In the twenty-first century, science has demonstrated that vitamin A greatly affects the immune system. What we are still lacking are clinical trials investigating the proper doses of vitamin A required to help ward off infectious disease and how large of an effect vitamin A supplementation has on populations that are not deficient in this . This brings up one of our common themes in this text—micronutrient deficiencies may contribute to the development, progression, and severity of a disease, but this does not mean that an increased intake of these will solely prevent or cure disease. The effect, as usual, is cumulative and depends on the diet as a whole, among other things.
Growth and Development
Vitamin A acts similarly to some hormones in that it is able to change the amount of proteins in cells by interacting with DNA. This is the primary way that vitamin A affects growth and development. Vitamin A deficiency in children is linked to growth retardation; however, vitamin A deficiency is often accompanied by protein malnutrition and iron deficiency, thereby confounding the investigation of vitamin A’s specific effects on growth and development.
In the fetal stages of life, vitamin A is important for limb, heart, eye, and ear development and in both deficiency and excess, vitamin A causes birth defects. Furthermore, both males and females require vitamin A in the diet to effectively reproduce.
Cancer
Vitamin A’s role in regulating cell growth and death, especially in tissues that line and cover organs, suggests it may be effective in treating certain cancers of the lung, neck, and liver. It has been shown in some observational studies that vitamin A-deficient populations have a higher risk for some cancers. However, vitamin A supplements have actually been found to increase the risk of lung cancer in people who are at high risk for the disease (i.e., smokers, ex-smokers, workers exposed to asbestos). The Beta-Carotene and Retinol Efficacy Trial (CARET) involving over eighteen thousand participants who were at high risk for lung cancer found that people who took supplements containing very high doses of vitamin A (25,000 international units) and beta-carotene had a 28 percent higher incidence of lung cancer midway through the study, which was consequently stopped.[2]
Vitamin A Toxicity
Vitamin A toxicity, or hypervitaminosis A, is rare. Typically it requires you to ingest ten times the of preformed vitamin A in the form of supplements (it would be hard to consume such high levels from a regular diet) for a substantial amount of time, although some people may be more susceptible to vitamin A toxicity at lower doses. The signs and symptoms of vitamin A toxicity include dry, itchy skin, loss of appetite, swelling of the brain, and joint pain. In severe cases, vitamin A toxicity may cause liver damage and coma.
Vitamin A is essential during pregnancy, but doses above 3,000 micrograms per day (10,000 international units) have been linked to an increased incidence of birth defects. Pregnant women should check the amount of vitamin A contained in any prenatal or pregnancy multivitamin she is taking to assure the amount is below the .
Dietary Reference Intakes for Vitamin A
There is more than one source of vitamin A in the diet. There is preformed vitamin A, which is abundant in many animal-derived foods, and there are carotenoids, which are found in high concentrations in vibrantly colored fruits and vegetables and some oils.
Some carotenoids are converted to retinol in the body by intestinal cells and liver cells. However, only minuscule amounts of certain carotenoids are converted to retinol, meaning fruits and vegetables are not necessarily good sources of vitamin A.
The RDA for vitamin A includes all sources of vitamin A. The RDA for vitamin A is given in mcg of Retinol Activity Equivalent () to take into account the many different forms it is available in. The human body converts all dietary sources of vitamin A into retinol. Therefore, 1 mcg of retinol is equivalent to 12 mcg of beta-carotene, and 24 mcg of alpha-carotene or beta-cryptoxanthin. For example, 12 micrograms of fruit- or vegetable-based beta-carotene will yield 1 microgram of retinol. Currently vitamin A listed in food and on supplement labels use international units (IUs). The following conversions are listed below[3]:
- 1 IU retinol = 0.3 mcg RAE
- 1 IU beta-carotene from dietary supplements = 0.15 mcg RAE
- 1 IU beta-carotene from food = 0.05 mcg RAE
- 1 IU alpha-carotene or beta-cryptoxanthin = 0.025 mcg RAE
The RDA for vitamin A is considered sufficient to support growth and development, reproduction, vision, and function while maintaining adequate stores (good for four months) in the liver.
Table 9.1 Dietary Reference Intakes for Vitamin A
| Age Group | RDA Males and Females mcg RAE/day | UL |
| Infants (0–6 months) | 400* | 600 |
| Infants (7–12 months) | 500* | 600 |
| Children (1–3 years) | 300 | 600 |
| Children (4–8 years) | 400 | 900 |
| Children (9–13 years) | 600 | 1,700 |
| Adolescents (14–18 years) | Males: 900 | 2,800 |
| Adolescents (14–18 years) | Females: 700 | 2,800 |
| Adults (> 19 years) | Males: 900 | 3,000 |
| Adults (> 19 years) | Females: 700 | 3,000 |
| *denotes Adequate Intake |
Source: Source: Dietary Supplement Fact Sheet: Vitamin A. National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminA-QuickFacts/. Updated September 5, 2012. Accessed October 7, 2017.
Dietary Sources of Vitamin A and Beta-Carotene
Preformed vitamin A is found only in foods from animals, with the liver being the richest source because that’s where vitamin A is stored (see Table 9.2 “Vitamin A Content of Various Foods”). The dietary sources of carotenoids will be given in the following text.
Table 9.2 Vitamin A Content of Various Foods
| Food | Serving | Vitamin A (IU) | Percent Daily Value |
| Beef liver | 3 oz. | 27,185 | 545 |
| Chicken liver | 3 oz. | 12,325 | 245 |
| Milk, skim | 1 c. | 500 | 10 |
| Milk, whole | 1 c. | 249 | 5 |
| Cheddar cheese | 1 oz. | 284 | 6 |
Source: Dietary Supplement Fact Sheet: Vitamin A. National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminA-QuickFacts/. Updated September 5, 2012. Accessed October 7, 2017.
In the United States, the most consumed carotenoids are alpha-carotene, beta-carotene, beta-cryptoxanthin, lycopene, lutein, and zeaxanthin. See Table 9.3 “Alpha- and Beta-Carotene Content of Various Foods” for the carotenoid content of various foods.
Table 9.3 Alpha- and Beta-Carotene Content of Various Foods
| Food | Serving | Beta-carotene (mg) | Alpha-carotene (mg) |
| Pumpkin, canned | 1c. | 17.00 | 11.70 |
| Carrot juice | 1c. | 22.00 | 10.20 |
| Carrots, cooked | 1c. | 13.00 | 5.90 |
| Carrots, raw | 1 medium | 5.10 | 2.10 |
| Winter squash, baked | 1c. | 5.70 | 1.40 |
| Collards, cooked | 1c. | 11.60 | 0.20 |
| Tomato | 1 medium | 0.55 | 0.10 |
| Tangerine | 1 medium | 0.13 | 0.09 |
| Peas, cooked | 1c. | 1.20 | 0.09 |
Source:2010. USDA National Nutrient Database for Standard Reference, Release 23. US Department of Agriculture, Agricultural Research Service. http://www.ars.usda.gov/ba/bhnrc/ndl. Accessed October 22, 2017.
Vitamin D Functions and Health Benefits
refers to a group of fat-soluble vitamins derived from cholesterol. Vitamins D2 (ergocalciferol) and D3 (calcitriol) are the only ones known to have biological actions in the human body. The skin synthesizes vitamin D when exposed to sunlight. In fact, for most people, more than 90 percent of their vitamin D3 comes from the casual exposure to the UVB rays in sunlight. Anything that reduces your exposure to the sun’s UVB rays decreases the amount of vitamin D3 your skin synthesizes. That would include long winters, your home’s altitude, whether you are wearing sunscreen, and the color of your skin (including tanned skin). Do you ever wonder about an increased risk for skin cancer by spending too much time in the sun? Do not fret. Less than thirty minutes of sun exposure to the arms and legs will increase blood levels of vitamin D3 more than orally taking 10,000 IU (250 micrograms) of vitamin D3.
Figure 9.5 The Functions of Vitamin D
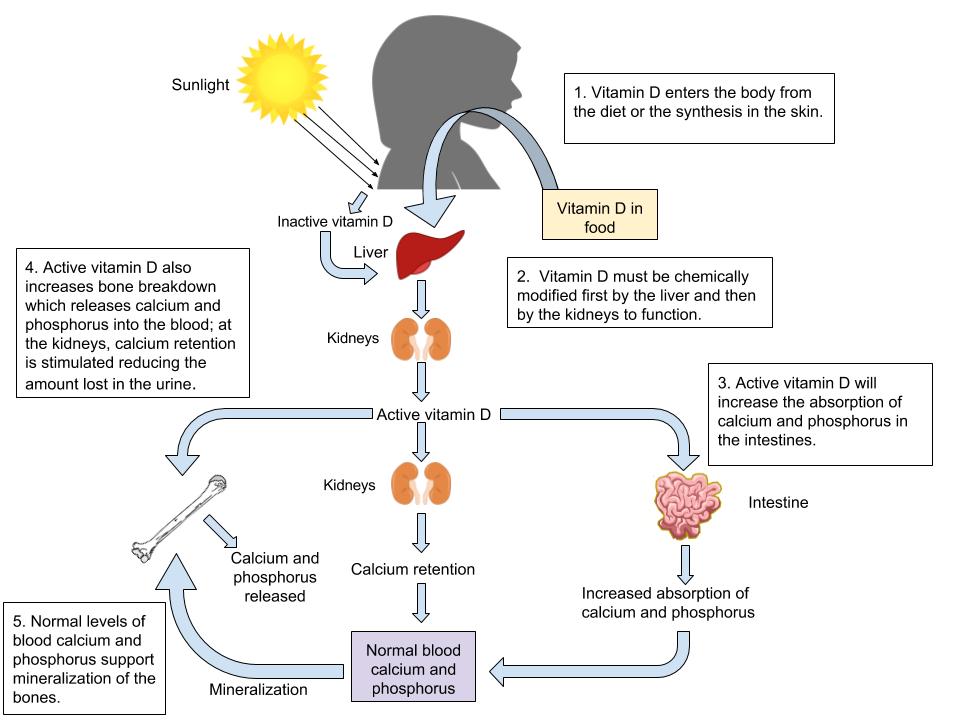
Vitamin D’s Functional Role
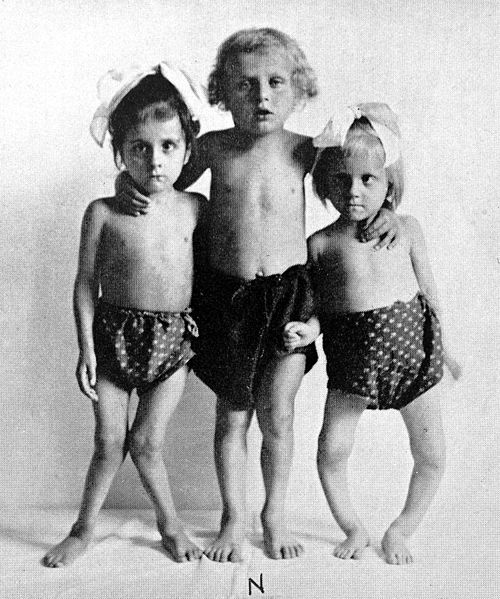
Activated vitamin D3 (calcitriol) regulates blood calcium levels in concert with . In the absence of an adequate intake of vitamin D, less than 15 percent of calcium is absorbed from foods or supplements. The effects of calcitriol on calcium homeostasis are critical for bone health. A deficiency of vitamin D in children causes the bone disease nutritional . Rickets is very common among children in developing countries and is characterized by soft, weak, deformed bones that are exceptionally susceptible to fracture. In adults, vitamin D deficiency causes a similar disease called , which is characterized by low BMD. Osteomalacia has the same symptoms and consequences as and often coexists with osteoporosis. Vitamin D deficiency is common, especially in the elderly population, dark-skinned populations, and in the many people who live in the northern latitudes where sunlight exposure is much decreased during the long winter season.
Figure 9.6 Rickets in Children
Health Benefits
Observational studies have shown that people with low levels of vitamin D in their blood have lower BMD and an increased incidence of osteoporosis. In contrast, diets with high intakes of salmon, which contains a large amount of vitamin D, are linked with better bone health. A review of twelve clinical trials, published in the May 2005 issue of the Journal of the American Medical Association, concluded that oral vitamin D supplements at doses of 700–800 international units per day, with or without coadministration of calcium supplements, reduced the incidence of hip fracture by 26 percent and other nonvertebral fractures by 23 percent.[4] A reduction in fracture risk was not observed when people took vitamin D supplements at doses of 400 international units.
Many other health benefits have been linked to higher intakes of vitamin D, from decreased cardiovascular disease to the prevention of infection. Furthermore, evidence from laboratory studies conducted in cells, tissues, and animals suggest vitamin D prevents the growth of certain cancers, blocks inflammatory pathways, reverses , increases secretion, and blocks viral and bacterial infection and many other things. Vitamin D deficiency has been linked to an increased risk for autoimmune diseases. Immune diseases, rheumatoid arthritis, multiple sclerosis, and Type 1 diabetes have been observed in populations with inadequate vitamin D levels. Additionally, vitamin D deficiency is linked to an increased incidence of . Until the results come out from the VITAL study, the bulk of scientific evidence touting other health benefits of vitamin D is from laboratory and observational studies and requires confirmation in clinical intervention studies.
Vitamin D Toxicity
Although vitamin D toxicity is rare, too much can cause high levels of calcium concentrations or hypercalcemia. Hypercalcemia can lead to a large amount of calcium to be excreted through the urine which can cause kidney damage. Calcium deposits may also develop in soft tissues such as the kidneys, blood vessels, or other parts of the . However, it is important to know that the synthesis of vitamin D from the sun does not cause vitamin D toxicity due to the skin production of vitamin D3 being a tightly regulated process.
Dietary Reference Intake for Vitamin D
The Institute of Medicine RDAs for vitamin D for different age groups is listed in Table 10.4 “Dietary Reference Intakes for Vitamin D”. For adults, the RDA is 600 international units (IUs), which is equivalent to 15 micrograms of vitamin D. The National Osteoporosis Foundation recommends slightly higher levels and that adults under age fifty get between 400 and 800 international units of vitamin D every day, and adults fifty and older get between 800 and 1,000 international units of vitamin D every day. According to the IOM, the tolerable upper intake level (UL) for vitamin D is 4,000 international units per day. Toxicity from excess vitamin D is rare, but certain diseases such as hyperparathyroidism, lymphoma, and tuberculosis make people more sensitive to the increases in calcium caused by high intakes of vitamin D.
Table 9.4 Dietary Reference Intakes for Vitamin D
| Age Group | RDA (mcg/day) | UL (mcg/day) |
| Infant (0–6 months) | 10* | 25 |
| Infants (6–12 months) | 10* | 25 |
| Children (1–3 years) | 15 | 50 |
| Children (4–8 years) | 15 | 50 |
| Children (9–13 years) | 15 | 50 |
| Adolescents (14–18 years) | 15 | 50 |
| Adults (19–71 years) | 15 | 50 |
| Adults (> 71 years) | 20 | 50 |
| * denotes Adequate Intake |
Source: Ross, A. C. et al. (2011). The 2011 Report on Dietary Reference Intakes for Calcium and Vitamin D from the Institute of Medicine: What Clinicians Need to Know. Journal of Clinical Endocrinology & Metabolism, 96(1), 53–8. http://www.ncbi.nlm.nih.gov/pubmed/21118827. Accessed October 10, 2017.
Dietary Sources of Vitamin D
Table 9.5 Vitamin D Content of Various Foods
| Food | Serving | Vitamin D (IU) | Percent Daily Value |
| Swordfish | 3 oz. | 566 | 142 |
| Salmon | 3 oz. | 447 | 112 |
| Tuna fish, canned in water, drained | 3 oz. | 154 | 39 |
| Orange juice fortified with vitamin D | 1 c. | 137 | 34 |
| Milk, nonfat, reduced fat, and whole, vitamin D- fortified | 1 c. | 115-124 | 29-31 |
| Margarine, fortified | 1 tbsp. | 60 | 15 |
| Sardines, canned in oil, drained | 2 e. | 46 | 12 |
| Beef liver | 3 oz. | 42 | 11 |
| Egg, large | 1 e. | 41 | 10 |
Source: Dietary Supplement Fact Sheet: Vitamin D. National Institutes of Health, Office of Dietary Supplements.https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/#h3. Updated September 5, 2012. Accessed October 22, 2017.
Vitamin E Functions and Health Benefits
occurs in eight chemical forms, of which appears to be the only form that is recognized to meet human requirements. Alpha-tocopherol and vitamin E’s other constituents are fat-soluble and primarily responsible for protecting cell membranes against lipid destruction caused by free radicals, therefore making it an antioxidant. When alpha-tocopherol interacts with a free radical it is no longer capable of acting as an antioxidant unless it is enzymatically regenerated. helps to regenerate some of the alpha-tocopherol, but the remainder is eliminated from the body. Therefore, to maintain vitamin E levels, you ingest it as part of your diet.
Insufficient levels are rare (signs and symptoms of such conditions are not always evident) but are primarily the result of nerve degeneration. People with malabsorption disorders, such as Crohn’s disease or cystic fibrosis, and babies born prematurely, are at higher risk for vitamin E deficiency.
Vitamin E has many other important roles and functions in the body such as boosting the by helping to fight off bacteria and viruses. It also enhances the dilation of blood vessels and inhibiting the formation of blood clotting. Despite vitamin E’s numerous beneficial functions when taken in recommended amounts, large studies do not support the idea that taking higher doses of this vitamin will increase its power to prevent or reduce disease risk.[5][6]
Fat in the diet is required for vitamin E absorption as it is packaged into lipid-rich chylomicrons in intestinal cells and transported to the liver. The liver stores some of the vitamin E or packages it into lipoproteins, which deliver it to cells.
Cardiovascular Disease
Vitamin E reduces the oxidation of LDLs, and it was therefore hypothesized that vitamin E supplements would protect against atherosclerosis. However, large clinical trials have not consistently found evidence to support this hypothesis. In fact, in the “Women’s Angiographic Vitamin and Estrogen Study,” postmenopausal women who took 400 international units (264 milligrams) of vitamin E and 500 milligrams of vitamin C twice per day had higher death rates from all causes.[7]
Other studies have not confirmed the association between increased vitamin E intake from supplements and increased mortality. There is more consistent evidence from observational studies that a higher intake of vitamin E from foods is linked to a decreased risk of dying from a heart attack.
Cancer
The large clinical trials that evaluated whether there was a link between vitamin E and cardiovascular disease risk also looked at cancer risk. These trials, called the HOPE-TOO Trial and Women’s Health Study, did not find that vitamin E at doses of 400 international units (264 milligrams) per day or 600 international units (396 milligrams) every other day reduced the risk of developing any form of cancer.[8][9]
Eye Conditions
plays a role in age-related loss of vision, called . Age-related macular degeneration (AMD) primarily occurs in people over age fifty and is the progressive loss of central vision resulting from damage to the center of the retina, referred to as the macula. There are two forms of AMD, dry and wet, with wet being the more severe form.
In the dry form, deposits form in the macula; the deposits may or may not directly impair vision, at least in the early stages of the disease. In the wet form, abnormal blood vessel growth in the macula causes vision loss. Clinical trials evaluating the effects of vitamin E supplements on AMD and cataracts (clouding of the lens of an eye) did not consistently observe a decreased risk for either. However, scientists do believe vitamin E in combination with other antioxidants such as zinc and copper may slow the progression of macular degeneration in people with early-stage disease.
Dementia
The brain’s high consumption makes it more vulnerable than other organs to oxidative stress. Oxidative stress has been implicated as a major contributing factor to and . Some studies suggest vitamin E supplements delay the progression of Alzheimer’s disease and cognitive decline, but again, not all of the studies confirm the relationship. A recent study with over five thousand participants published in the July 2010 issue of the Archives of Neurology demonstrated that people with the highest intakes of dietary vitamin E were 25 percent less likely to develop dementia than those with the lowest intakes of vitamin E.[10]
More studies are needed to better assess the dose and dietary requirements of vitamin E and, for that matter, whether other antioxidants lower the risk of dementia, a disease that not only devastates the mind, but also puts a substantial burden on loved ones, caretakers, and society in general.
Vitamin E Toxicity
Currently, researchers have not found any adverse effects from consuming vitamin E in food. Although that may be the case, supplementation of alpha-tocopherol in animals has shown to cause hemorrhage and disrupt blood coagulation. Extremely high levels of vitamin E can interact with -dependent clotting factors causing an inhibition of blood clotting.[11]
Dietary Reference Intakes for Vitamin E
The Recommended Dietary Allowances (RDAs) and Tolerable Upper Intake Levels (ULs) for different age groups for vitamin E are given in Table 9.6 “Dietary Reference Intakes for Vitamin E”.
Table 9.6 Dietary Reference Intakes for Vitamin E
| Age Group | RDA Males and Females mg/day | UL |
| Infants (0–6 months) | 4* | – |
| Infants (7–12 months) | 5* | – |
| Children (1–3 years) | 6 | 200 |
| Children (4–8 years) | 7 | 300 |
| Children (9–13 years) | 11 | 600 |
| Adolescents (14–18 years) | 15 | 800 |
| Adults (> 19 years) | 15 | 1,000 |
| *denotes Adequate Intake |
Source: Dietary Supplement Fact Sheet: Vitamin E.National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminE-QuickFacts/. Updated October 11, 2011. Accessed October 5, 2017.
Vitamin E supplements often contain more than 400 international units, which is almost twenty times the RDA. The UL for vitamin E is set at 1,500 international units for adults. There is some evidence that taking vitamin E supplements at high doses has negative effects on health. As mentioned, vitamin E inhibits blood clotting and a few clinical trials have found that people taking vitamin E supplements have an increased risk of stroke. In contrast to vitamin E from supplements, there is no evidence that consuming foods containing vitamin E compromises health.
Dietary Sources of Vitamin E
Add some nuts to your salad and make your own dressing to get a healthy dietary dose of vitamin E.

Vitamin E is found in many foods, especially those higher in fat, such as nuts and oils. Some spices, such as paprika and red chili pepper, and herbs, such as oregano, basil, cumin, and thyme, also contain vitamin E. (Keep in mind spices and herbs are commonly used in small amounts in cooking and therefore are a lesser source of dietary vitamin E.) See Table 10.7 “Vitamin E Content of Various Foods” for a list of foods and their vitamin E contents.
Everyday Connection
To increase your dietary intake of vitamin E from plant-based foods try a spinach salad with tomatoes and sunflower seeds, and add a dressing made with sunflower oil, oregano, and basil.
Table 9.7 Vitamin E Content of Various Foods
| Food | Serving Size | Vitamin E (mg) | Percent Daily Value |
| Sunflower seeds | 1 oz. | 7.4 | 37 |
| Almonds | 1 oz. | 6.8 | 34 |
| Sunflower oil | 1 Tbsp | 5.6 | 28 |
| Hazelnuts 1 oz. | 1 oz. | 4.3 | 22 |
| Peanut butter | 2 Tbsp. | 2.9 | 15 |
| Peanuts 1 oz. | 1 oz. | 2.2 | 11 |
| Corn oil 1 Tbsp. | 1 Tbsp. | 1.9 | 10 |
| Kiwi | 1 medium | 1.1 | 6 |
| Tomato | 1 medium | 0.7 | 4 |
| Spinach | 1 c. raw | 0.6 | 3 |
Source: Dietary Supplement Fact Sheet: Vitamin E.National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminE-QuickFacts/. Updated October 11, 2011. Accessed October 5, 2017.
Vitamin K Functions and Health Benefits
Vitamin K refers to a group of fat-soluble vitamins that are similar in chemical structure. Vitamin K is critical for blood function acting as which play an essential role in blood coagulation (aka blood clotting). Blood-clotting proteins are continuously circulating in the blood. Upon injury to a blood vessel, platelets stick to the wound forming a plug. Without vitamin K, blood would not clot.
A deficiency in vitamin K causes bleeding disorders. It is relatively rare, but people who have liver or pancreatic disease, celiac disease, or malabsorption conditions are at higher risk for vitamin K deficiency. Signs and symptoms include nosebleeds, easy bruising, broken blood vessels, bleeding gums, and heavy menstrual bleeding in women. The function of the anticoagulant drug warfarin is impaired by excess vitamin K intake from supplements. Calcium additionally plays a role in activation of blood-clotting proteins.
Bone Health
Vitamin K is also required for maintaining bone health. It modifies the protein osteocalcin, which is involved in the process. All the functions of osteocalcin and the other vitamin K-dependent proteins in are not well understood and are under intense study. Some studies do show that people who have diets low in vitamin K also have an increased risk for bone fractures.
Dietary Reference Intake and Food Sources for Vitamin K
The of vitamin K for adult females is 90 micrograms per day, and for males it is 120 micrograms per day. A UL for vitamin K has not been set. The Food and Nutrition Board (FNB) has not established an UL for vitamin K because it has a low potential for toxicity. According to the FNB, “no adverse effects associated with vitamin K consumption from food or supplements have been reported in humans or animals.”
Institute of Medicine. Dietary reference intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. Washington, DC: National Academy Press; 2001.
Table 9.8 Dietary Reference Intakes for Vitamin K
| Age Group | RDA (mcg/day) |
| Infants (0–6 months) | 2.0* |
| Infants (6–12 months) | 2.5* |
| Children (1–3 years) | 30 |
| Children (4–8 years) | 55 |
| Children (9–13 years) | 60 |
| Adolescents (14–18 years) | 75 |
| Adult Males (> 19 years) | 120 |
| Adult Females (> 19 years) | 90 |
| * denotes Adequate Intake |
Source: Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. Institute of Medicine. http://www.iom.edu/Reports/2001/Dietary-Reference-Intakes-for-Vitamin-A-Vitamin-K-Arsenic-Boron-Chromium-Copper-Iodine-Iron-Manganese-Molybdenum-Nickel-Silicon-Vanadium-and-Zinc.aspx. Published January 9, 2001. Accessed October 10, 2017.
Dietary Sources of Vitamin K
Vitamin K is present in many foods. It is found in highest concentrations in green vegetables such as broccoli, cabbage, kale, parsley, spinach, and lettuce. Additionally, vitamin K can be synthesized via bacteria in the large intestine. The exact amount of vitamin K synthesized by bacteria that is actually absorbed in the lower intestine is not known, but likely contributes less than 10 percent of the recommended intake. Newborns have low vitamin K stores and it takes time for the sterile newborn gut to acquire the good bacteria it needs to produce vitamin K. So, it has become a routine practice to inject newborns with a single intramuscular dose of vitamin K. This practice has basically eliminated vitamin K-dependent bleeding disorders in babies.
Table 9.9 Dietary Sources of Vitamin K
| Food | Serving | Vitamin K (mcg) | Percent Daily Value |
| Broccoli | ½ c. | 160 | 133 |
| Asparagus | 4 spears | 34 | 28 |
| Cabbage | ½ c. | 56 | 47 |
| Spinach | ½ c. | 27 | 23 |
| Green peas | ½ c. | 16 | 13 |
| Cheese | 1 oz. | 10 | 8 |
| Ham | 3 oz. | 13 | 11 |
| Ground beef | 3 oz. | 6 | 5 |
| Bread | 1 slice | 1.1 | <1 |
| Orange | 1 e. | 1.3 | 1 |
Summary of Fat-soluble Vitamins
Table 9.10 Fat-Soluble Vitamins
| Vitamin | Sources | Recommended Intake for adults | Major functions | Deficiency diseases and symptoms | Groups at risk of deficiency | Toxicity | UL |
| Vitamin A (retinol, retinal, retinoic acid,carotene, beta-carotene) | Retinol: beef and chicken liver, skim milk, whole milk, cheddar cheese; Carotenoids: pumpkin, carrots, squash, collards, peas | 700-900 mcg/day | Antioxidant,vision, cell differentiation, reproduction, immune function | Xerophthalmia, night blindness, eye infections; poor growth, dry skin, impaired immune function | People living in poverty (especially infants and children), premature infants, pregnant and lactating women people who consume low-fat or low-protein diets | Hypervitaminosis A: Dry, itchy skin, hair loss, liver damage, joint pain, fractures, birth defects, swelling of the brain | 3000 mcg/day |
| Vitamin D | Swordfish, salmon, tuna, orange juice (fortified), milk (fortified), sardines, egg, synthesis from sunlight | 600-800 IU/day (15-20 mcg/day) | Absorption and regulation of calcium and phosphorus, maintenance of bone | Rickets in children: abnormal growth, misshapen bones, bowed legs, soft bones; osteomalacia in adults | Breastfed infants, older adults people with limited sun exposure, people with dark skin | Calcium deposits in soft tissues, damage to the heart, blood vessels, and kidneys | 4000 IU/day (100 mcg/day) |
| Vitamin E | Sunflower seeds, almonds, hazelnuts,peanuts | 15 mg/day | Antioxidant, protects cell membranes | Broken red blood cells, nerve damage | People with poor fat absorption, premature infants | Inhibition of vitamin K clotting factors | 1000 mcg/day from supplemental sources |
| Vitamin K | Vegetable oils, leafy greens, synthesis by intestinal bacteria | 90-120 mcg/day | Synthesis of blood clotting proteins and proteins needed for bone health and cell growth | Hemorrhage | Newborns, people on long term antibiotics | Anemia, brain damage | ND |
Learning Activities
Technology Note: The second edition of the Human Nutrition Open Educational Resource (OER) textbook features interactive learning activities. These activities are available in the web-based textbook and not available in the downloadable versions (EPUB, Digital PDF, Print_PDF, or Open Document).
Learning activities may be used across various mobile devices, however, for the best user experience it is strongly recommended that users complete these activities using a desktop or laptop computer and in Google Chrome.
- Sommer A. (2008). Vitamin A Deficiency and Clinical Disease: An Historical Overview. Journal of Nutrition, 138, 1835–39. http://jn.nutrition.org/content/138/10/1835.long. Accessed October 4, 2017. ↵
- Goodman GE, et al. (2004). The Beta-Carotene and Retinol Efficacy Trial: Incidence of Lung Cancer and Cardiovascular Disease Mortality During 6-year Follow-up after Stopping Beta-Carotene and Retinol Supplements. Journal of the National Cancer Institute, 96(23), 1743–50. http://jnci.oxfordjournals.org/content/96/23/1743.long. Accessed October 6, 2017. ↵
- Dietary Supplement Fact Sheet: Vitamin A. National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminA-QuickFacts/. Updated September 5, 2012. Accessed October 7, 2017. ↵
- Bischoff-Ferrari, HA, et al. (2005). Fracture Prevention with Vitamin D Supplementation: A Meta-Analysis of Randomized Controlled Trials. Journal of the American Medical Association, 293(18), 2257–64. http://jama.ama-assn.org/content/293/18/2257.long. Accessed October 12, 2017. ↵
- Goodman M, Bostlick RM, Kucuk O, Jones DP. (2011). Clinical trials of antioxidants as cancer prevention agents: past, present, and future. Free Radical Biology & Medicine, 51(5), 1068–84. https://www.ncbi.nlm.nih.gov/pubmed/21683786. Accessed October 5, 2017. ↵
- McGinley C, Shafat A. Donnelly AE. (2009). Does antioxidant vitamin supplementation protect against muscle damage. Sports Medicine, 39(12), 1011–32. https://www.ncbi.nlm.nih.gov/pubmed/19902983. Accessed October 5, 2017. ↵
- Waters DD, et al. (2002). Effects of Hormone Replacement Therapy and Antioxidant Vitamin Supplements on Coronary Atherosclerosis in Postmenopausal Women: A Randomized Controlled Trial. The Journal of the American Medical Association, 288(19), 2432–40. https://jamanetwork.com/journals/jama/fullarticle/195531. Accessed October 5, 2017. ↵
- HOPE and HOPE-TOO Trial Investigators. (2005). Effects of Long-Term Vitamin E Supplementation on Cardiovascular Events and Cancer. The Journal of the American Medical Association, 293, 1338–47. http://jama.ama-assn.org/content/293/11/1338.long., Accessed October 5, 2017. ↵
- Lee IM, et al. (2005). Vitamin E in the Primary Prevention of Cardiovascular Disease and Cancer: The Women’s Health Study. The Journal of the American Medical Association, 294, 56–65. http://jama.ama-assn.org/content/294/1/56.long. Accessed October 5, 2017. ↵
- Devore EE, et al. (2010). Dietary Antioxidants and Long-Term Risk of Dementia, Archives of Neurology, 67(7), 819–25. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2923546/?tool=pubmed. Accessed October 5, 2017. ↵
- Dietary Supplement Fact Sheet: Vitamin E.National Institutes of Health, Office of Dietary Supplements. http://ods.od.nih.gov/factsheets/VitaminE-QuickFacts/. Updated October 11, 2011. Accessed October 5, 2017. ↵
A fat-soluble vitamin that is needed for cell differentiation, reproduction, and vision.
Forms of preformed vitamin A.
Vitamin A in its alcohol form.
Vitamin A in its aldehyde form.
A class of retinoids that can serve as precursors of vitamin A.
A carotenoid that can be cleaved to release two retinol molecules.
A carotenoid that is found in most plant foods like leafy green vegetables, carrots, and squash.
A carotenoid that is found in most plant foods like corn, green peppers, and lemon.
Compounds that inhibit the oxidation of other substances.
A substance that does not dissolve in water. Examples include triglycerides and vitamins A, D, E & K.
The lowest density lipoprotein particles which contain triglycerides, monoglycerides, and small amounts of cholesterol and phospholipids.
A protein that is essential for the transport of vitamin A from the liver to the tissues in need.
A condition due to a deficiency in vitamin A where the eye recovers very slowly from exposure to bright light.
A major antioxidant that prevents damage to important cellular components caused by reactive oxygen species
A highly reactive atom or molecule that causes oxidative damage.
An advanced form of eye lesions resulting from vitamin A deficiency.
Organic compounds that are needed in small amounts in the diet to support and regulate the chemical reactions and processes needed for growth, reproduction, and the maintenance of health.
Essential nutrients that are needed by the body in small amounts. These include vitamins and minerals.
(Recommended Dietary Allowance) The levels of intake of essential nutrients that is based off of scientific knowledge, and it judged by the Food and Nutrition Board to be adequate to meet the known nutrient needs for all healthy people.
(Tolerable Upper Intake Level) The maximum daily nutrient intake levels that are likely to pose health risks to almost all individuals in a given gender and life-stage group.
(Retinol Activity Equivalent) The amount of retinol, alpha-carotene, beta-carotene, or beta-cryptoxanthin that must be consumed to equal 1 mcg of retinol.
Comprised of several types of white blood cells that circulate in the blood and lymph. Jobs are to seek, recruit, attack, and destroy foreign invaders, such as bacteria and viruses.
A fat-soluble vitamin that can be made in the body when there is exposure to sunlight and is needed for the absorption of calcium.
A hormone that acts to increase blood calcium levels and is released from the parathyroid gland.
A disease that is characterized by softening of the bones due to poor calcium deposition within them because of a lack of vitamin D in the body.
A disease that is characterized by defective bone formation that may be due to a vitamin D deficiency or a lack of sunlight exposure.
A disorder affecting the bones that is characterized as a loss in bone mass, increased bone fragility, and increased risk of fractures.
The thickening of artery walls which is caused by the growth of hard deposits containing lipids and other materials.
A hormone secreted by the pancreas in response to elevated blood glucose levels to transport glucose into the muscle or fat cells.
Abnormally high blood pressure.
The organ system that includes the heart and blood vessels that circulates blood throughout the body.
A fat-soluble vitamin that functions as an antioxidant in the body.
The active form of vitamin E in humans.
A water soluble vitamin that is needed for the maintenance of collagen.
Damage resulting from an imbalance between oxidative oxygen molecules and antioxidant defenses.
The deterioration of a portion of the retina that results in loss of visual detail and eventually blindness.
A 6-carbon monosaccharide that is the major carbohydrate used to provide energy in the body.
The deterioration of an individual’s mental state that results in impaired memory, thinking, and judgement.
A disease that results in an irreversible loss of mental function.
A fat-soluble vitamin that is needed for blood clotting.
Chemical groups that bind to enzymes and assist in enzymatic catalysis.
A process where bone is continuously being broken down and reformed for growth and maintenance.
The major structural and supportive connective tissue of the body.
(Adequate Intake) The level of nutrient intake that should be used as a goal when no RDA exists. This value is an approximation of the nutrient intake that sustains health.

{kind=link}
{kind=link}
{kind=link}